Understanding IBD: What Everyone Should Know About Crohn’s and UC

Picture this: you wake up feeling good, maybe even optimistic about the day ahead. Then, halfway through your morning coffee, that familiar cramping starts. The uncertainty hits like a wave—will today be manageable, or will you be counting bathroom locations between meetings? If you’re living with Crohn’s disease or ulcerative colitis, this scenario probably feels all too familiar.
The unpredictability of inflammatory bowel disease affects so much more than our digestive systems. It touches our relationships, our career choices, our travel plans, and even our most basic daily routines. Yet despite how common IBD is—affecting millions of people worldwide—many of us still feel isolated in our experience, wondering if anyone truly understands what we’re going through.
Summary of What Is Crohn’s Disease and Ulcerative Colitis?
Both Crohn’s disease and ulcerative colitis are forms of inflammatory bowel disease (IBD), conditions that cause chronic inflammation in the digestive tract. While they share many similarities, they have distinct differences that affect how they’re diagnosed and treated.
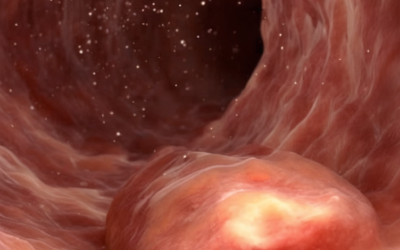
Crohn’s disease can occur anywhere along the digestive tract, from mouth to anus, and often appears in patches with healthy tissue in between. It affects all layers of the bowel wall. Ulcerative colitis, on the other hand, is limited to the colon and rectum, causes continuous inflammation starting from the rectum, and only affects the innermost lining of the colon.
Common symptoms include abdominal pain, cramping, frequent diarrhea, fatigue, and unintended weight loss. Some people also experience joint pain and skin problems. The severity and combination of symptoms varies significantly between individuals.
Experts believe IBD results from a combination of genetic predisposition, environmental factors, and immune system dysfunction. It’s important to understand that IBD isn’t caused by diet, stress, or lifestyle choices, and it’s not contagious. While stress and certain foods may worsen symptoms, they don’t cause the disease.
Treatment options have expanded considerably and include anti-inflammatory medications, immune system suppressors, and biologic therapies designed to reduce inflammation and control symptoms. Some patients may require surgery if medications aren’t effective. Lifestyle modifications, including dietary changes, regular exercise, and stress management, can significantly improve quality of life and help manage symptoms.
This post summarizes reporting from What Is Crohn’s Disease and Ulcerative Colitis?. Our analysis represents IBD Movement’s perspective and is intended to help patients understand how this news may affect them. Read the original article for complete details.
What This Means for the IBD Community
Understanding the fundamental differences between Crohn’s and ulcerative colitis isn’t just academic knowledge—it’s deeply personal information that can help you advocate for yourself and make sense of your own experience. When I talk with newly diagnosed patients, one of the first things they want to know is “why me?” The reality that IBD isn’t caused by something they did wrong often comes as both a relief and a frustration.
The fact that these conditions result from complex interactions between genetics, environment, and immune function helps explain why IBD can feel so unpredictable. Your flares aren’t happening because you’re not trying hard enough or because you ate the “wrong” thing. They’re the result of intricate biological processes that researchers are still working to fully understand.
This understanding can be liberating for many of us who’ve spent years wondering if we somehow brought this condition on ourselves. It also helps explain why what works for one person with IBD might not work for another, even if they have the same diagnosis. Your Crohn’s disease might behave completely differently from your friend’s Crohn’s, and that’s not unusual—it’s actually expected.
From a practical standpoint, knowing whether inflammation affects all layers of your bowel wall (as in Crohn’s) or just the inner lining (as in UC) can help you understand why certain treatments are recommended for you. It can also help you make sense of your symptoms and why your doctor might be monitoring specific complications.
The emphasis on multidisciplinary care teams resonates deeply with many of us who’ve learned that managing IBD effectively requires more than just medical treatment. The gastroenterologist who manages your medications, the dietitian who helps you identify trigger foods, the mental health counselor who helps you cope with the emotional aspects of chronic illness—they’re all essential pieces of your care puzzle.
Here are some questions this information might prompt you to discuss with your healthcare team:
- How extensive is my disease, and what does that mean for my long-term outlook?
- Are there specific complications I should watch for given my type of IBD?
- How might my disease pattern influence my treatment options?
- What role should diet and lifestyle modifications play in my specific case?
- How do we balance treating active inflammation with preventing future flares?
The evolution in IBD treatments mentioned in the article represents one of the most hopeful aspects of living with these conditions today. The fact that we have biologics, biosimilars, and increasingly targeted therapies means that even if your first treatment doesn’t work perfectly, you have options. This is a dramatically different landscape than what patients faced even a decade ago.
But perhaps most importantly, the acknowledgment that IBD affects us physically and emotionally validates what many of us have long known—that living with chronic illness requires support beyond just medical management. The mention of patient communities isn’t just a nice addition; for many of us, connecting with others who truly understand this experience has been transformative.
The unpredictability that defines IBD—never knowing how you’ll feel from one day to the next—creates a unique set of challenges that healthy people often struggle to comprehend. When friends and family read that IBD symptoms “vary widely from person to person,” it might help them understand why you can’t always predict how you’ll feel or why you might need to cancel plans at the last minute.
The Bottom Line
Living with IBD means living with uncertainty, but it doesn’t mean living without hope or control. Understanding your condition—whether it’s Crohn’s disease or ulcerative colitis—empowers you to be an active participant in your care and helps you make informed decisions about your health.
Remember that your IBD journey is uniquely yours. While the basic disease mechanisms might be similar to others with your condition, your experience, your triggers, your response to treatment, and your path forward will be individual. This isn’t something to be frustrated about—it’s actually a reminder that personalized care and self-advocacy are so important. You are the expert on your own body and experience, and that expertise, combined with good medical care and community support, can help you navigate this journey with greater confidence and hope.
IBD Movement provides information for educational purposes only. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.
Related Posts

New Research Links Certain Occupations to Higher IBD Risk: What This Means for Your Career and Health
February 28, 2026
Eli Lilly’s Omvoh Shows Promise for Crohn’s Disease: What This Breakthrough Could Mean for Your Treatment Journey
February 27, 2026
Could Your Cholesterol Medication Help Your IBD? New Research Reveals Surprising Connection
February 27, 2026