When Crohn’s Disease Masquerades as Another Condition: A Critical Lesson in Accurate Diagnosis
Summary of Unknown
IBD Movement provides news analysis and insights for the IBD community. Always consult your healthcare provider for personal medical advice.
For many of us living with Crohn’s disease, the journey to diagnosis can feel like navigating a medical maze. But what happens when even experienced healthcare providers are thrown off course? A recent case study reveals how Crohn’s disease can mimic other conditions so closely that it leads to misdiagnosis—with potentially life-threatening consequences. This sobering reminder underscores why getting the right diagnosis from the start is absolutely crucial for anyone experiencing unexplained gastrointestinal symptoms.
The Case That Highlights Diagnostic Challenges
According to the medical journal Cureus, researchers documented a complex case involving a 60-year-old Hispanic man whose symptoms initially pointed to Behçet’s disease rather than Crohn’s disease. The patient presented with a constellation of concerning symptoms: progressive weight loss, painful oral and genital ulcers, joint pain, and chronic diarrhea—all hallmarks that can appear in both conditions.
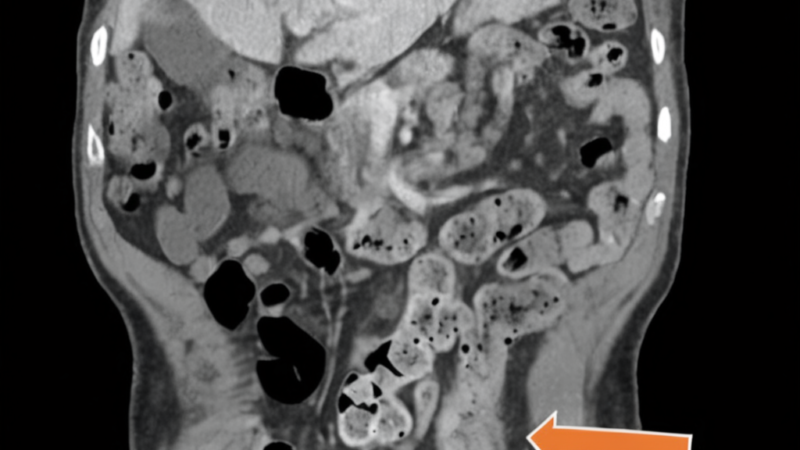
Initially treated for presumed Behçet’s disease with corticosteroids and immunomodulatory therapy, the patient experienced only partial improvement. Over several months, his condition deteriorated dramatically, culminating in severe abdominal pain and a life-threatening bowel perforation. Emergency surgery revealed the true diagnosis: Crohn’s colitis, not Behçet’s disease.
The diagnostic breakthrough came through histopathologic examination during surgery, which showed the characteristic transmural inflammation of Crohn’s disease without the vasculitis typically seen in Behçet’s disease. Following the correct diagnosis, the patient was started on infliximab therapy and achieved clinical stabilization.
What This Means for the IBD Community
This case study illuminates several critical issues that resonate deeply with anyone who has experienced the IBD diagnostic journey. First and foremost, it demonstrates how symptom overlap between different inflammatory conditions can create genuine diagnostic uncertainty, even among experienced medical professionals. This isn’t about medical incompetence—it’s about the inherent complexity of inflammatory diseases that share similar presentations.
For people with IBD, this case reinforces the importance of persistent advocacy for proper diagnostic workup. The patient in this study experienced months of inadequate treatment because the initial diagnosis was incorrect. While corticosteroids provided some temporary relief (as they often do for various inflammatory conditions), the underlying Crohn’s disease continued to progress, ultimately leading to a surgical emergency.
The progression to bowel perforation in this case is particularly sobering. Perforation represents one of the most serious complications of Crohn’s disease, occurring when inflammation weakens the intestinal wall to the point of rupture. This complication carries significant risks, including peritonitis, sepsis, and even death if not treated promptly. The fact that this patient’s perforation might have been prevented with earlier, appropriate IBD treatment underscores the stakes involved in accurate diagnosis.
This case also highlights the critical role of tissue biopsy and histopathologic examination in differentiating between similar conditions. While blood tests, imaging, and clinical presentation provide important clues, sometimes definitive diagnosis requires examining actual tissue samples under a microscope. For people with IBD, this reinforces why procedures like colonoscopy with biopsy remain the gold standard for diagnosis and monitoring.
The successful treatment with infliximab following correct diagnosis offers hope and demonstrates the effectiveness of targeted IBD therapies when properly applied. Infliximab, a TNF-alpha inhibitor, has revolutionized treatment for moderate to severe Crohn’s disease, often achieving remission in patients who haven’t responded to conventional therapies. This patient’s clinical stabilization on infliximab validates the importance of getting the right treatment for the right condition.
From a broader perspective, this case emphasizes the need for ongoing diagnostic reassessment when patients aren’t responding as expected to treatment. The medical team’s willingness to reconsider the diagnosis when the patient’s condition deteriorated likely saved his life. For patients, this reinforces the importance of maintaining open communication with healthcare providers about treatment response and any worsening symptoms.
The case also touches on the challenges faced by Hispanic and other minority populations in healthcare settings. While not explicitly discussed in the study, research has shown that diagnostic delays and misdiagnoses can be more common in underserved populations, making cases like this particularly important for highlighting the need for equitable, thorough diagnostic approaches for all patients.
Expert Perspective on Differential Diagnosis
Gastroenterologists and rheumatologists emphasize that distinguishing between Crohn’s disease and Behçet’s disease requires careful attention to subtle but important differences. While both conditions can cause oral ulcers, gastrointestinal symptoms, and systemic inflammation, Behçet’s disease typically involves ocular symptoms and characteristic skin lesions that weren’t present in this case.
Medical experts recommend that patients experiencing overlapping symptoms should seek evaluation at centers with experience in inflammatory bowel diseases. A multidisciplinary approach involving gastroenterology, rheumatology, and pathology can help ensure accurate diagnosis and appropriate treatment selection. Patients should feel empowered to ask their doctors about the diagnostic process and request second opinions when treatment isn’t providing expected results.
Key Takeaways for IBD Patients
- Advocate for comprehensive diagnostic workup: If you’re experiencing symptoms that could indicate IBD, ensure your healthcare team considers all possibilities and performs appropriate testing, including endoscopy with biopsy when indicated.
- Monitor treatment response closely: If you’re not improving on prescribed therapy, communicate this clearly to your healthcare team and don’t hesitate to ask whether the diagnosis should be reconsidered.
- Recognize emergency warning signs: Severe abdominal pain, especially if sudden or accompanied by fever, requires immediate medical attention as it could indicate complications like perforation.
- Seek specialized care: For complex cases or when diagnosis is uncertain, consider evaluation at a center specializing in inflammatory bowel diseases.
- Maintain detailed symptom records: Keep track of all symptoms, their timing, and response to treatments—this information can be crucial for accurate diagnosis.
Moving Forward with Confidence
While this case study presents a sobering reminder of diagnostic challenges, it ultimately demonstrates the resilience of both patients and the medical system. The patient’s successful treatment following correct diagnosis shows that even complex cases can have positive outcomes when the right approach is applied. For our IBD community, this case reinforces the importance of persistent advocacy, comprehensive care, and the hope that effective treatments await once we have the right diagnosis in hand.
As we continue to share experiences and support one another through the diagnostic journey, cases like this remind us why our voices matter and why we must continue pushing for excellence in IBD care. Every story shared helps build the knowledge base that can prevent others from experiencing similar diagnostic delays and complications.
Source: This post summarizes reporting from Unknown. Read the original article.